March 2025 Case Study
Nikita Menta, BA1, Nagasai Adusumilli, MD, MBA1
- Department of Dermatology, The George Washington University School of Medicine and Health Sciences
Patient History
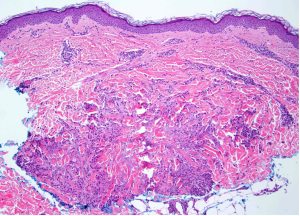
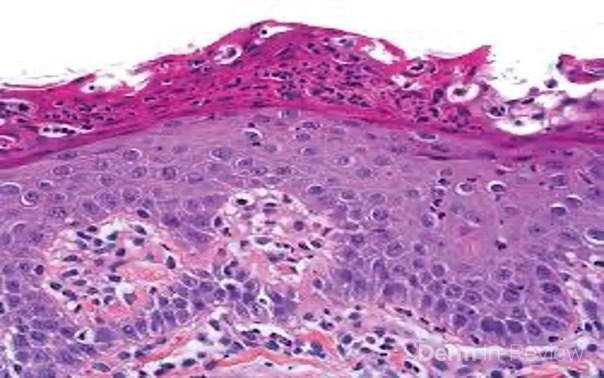
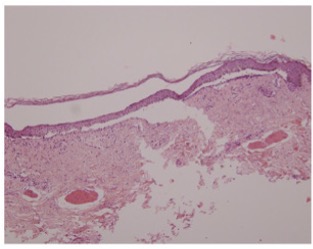
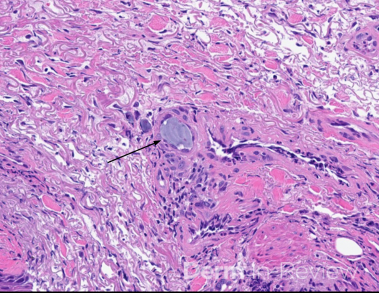
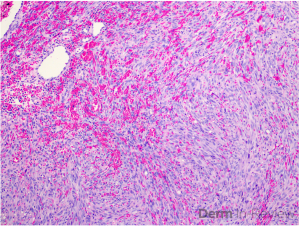
A 67-year-old female with a medical history of type II diabetes, breast cancer (s/p right mastectomy 15 years prior), and a 35-pack-year smoking history (quit 15 years prior) presented to the clinic with itchy, red, raised lesions on the arms, chest, and back. The rash started on the upper arms one year prior to presentation and gradually spread to involve the trunk At the time of presentation, the patient was undergoing workup of an enlarging solid pulmonary nodule. Exam findings are shown in Figure 1, and results from a punch biopsy of the left anterior shoulder stained with hematoxylin and eosin are shown in Figure 2.
Based on the clinical presentation and biopsy findings, which three features should elicit concern for underlying malignancy in a patient with this condition?
- Generalized Distribution
- Female Gender
- Age <60
- Localized Distribution
- Male Gender
- Age >60
- Symptomatic lesions
- Lack of response to systemic treatment


Correct Answer: 1, 6, 8
Explanation/Literature Review:
In the setting of an enlarging pulmonary nodule and extensive smoking history, the multiple pink-to-red annular plaques with central clearing, along with a biopsy demonstrating interstitial and perivascular lymphohistiocytic infiltrate with rare granulomas, is consistent with a diagnosis of paraneoplastic granuloma annulare (GA). Paraneoplastic GA is defined as GA that occurs within 6 months of malignancy diagnosis and/or GA that resolves with definitive cancer treatment.1 Paraneoplastic GA is a rare condition, and while large-scale epidemiologic studies quantifying prevalence are lacking, one study of 934 cases of generalized GA found that 3.5% were paraneoplastic.1 The pathogenesis of GA remains incompletely understood, though it is thought to be a delayed-type Th1-cell mediated hypersensitivity reaction to unidentified antigens.2,3 In paraneoplastic GA, specifically, it is hypothesized that either tumor antigens or cytokines secreted by the tumor trigger the hypersensitivity reaction.2,4 Paraneoplastic GA has been observed in association with multiple malignancy types – most commonly hematologic malignancies, followed by solid organ malignancies.5,6
Certain demographic, clinical, and histopathologic features have been reported more frequently in patients with paraneoplastic GA compared to classic GA. First, paraneoplastic GA most commonly occurs in older individuals, specifically those in their seventh to eighth decades of life (answer choice 6).6,7 In terms of clinical features, nearly all paraneoplastic GA cases are of the generalized subtype (answer choice 1), though localized paraneoplastic GA has been reported.7 As for histopathologic features, the interstitial, as opposed to the necrobiotic, histologic variant and higher degrees of perivascular lymphocytic infiltrate have both been reported more frequently in cases of paraneoplastic GA.6,7 Conversely, the presence of multinucleated giant cells and mucin has been observed in more cases of classic GA.6
There are no standardized guidelines for malignancy screening in patients with GA, however, if patients are above 60 years, present with generalized GA, and/or are unresponsive to systemic treatment, dermatologists should ensure that all age-appropriate and any patient-specific cancer screenings, based on individual risk factors, are up to date.7 Along these lines, if patients have a prior history of cancer, it is important to ensure that they are undergoing routine surveillance. Additionally, a thorough history and physical exam are critical for identifying any subtle symptoms or signs of underlying malignancy.7 In this patient, in addition to routine age-appropriate cancer screenings and breast cancer surveillance, a low-dose CT scan would have been indicated if she wasn’t already undergoing workup of her pulmonary nodule. Finally, management of paraneoplastic GA, from the dermatologist’s perspective, is relatively straightforward, as it is typically resistant to conventional local and systemic GA therapies (answer choice 8) but resolves within ~6 months of malignancy treatment.1,6 Accordingly, dermatologists’ efforts should be directed toward facilitating timely diagnosis and management of malignancy.
Incorrect answer choices:
Female Gender, Male Gender (2, 5) – While classic GA demonstrates a female gender predominance, no gender predominance has been identified in paraneoplastic GA.6,7
Age <60 (3) – Paraneoplastic GA most commonly occurs in individuals in their seventh to eighth decades of life. However, generalized GA, that is not associated with malignancy, peaks bimodally in the first and fifth decades of life.6
Localized Distribution (D) – While localized GA associated with malignancy has been reported, most paraneoplastic GA cases are of the generalized subtype.7
Symptomatic Lesions (G) – No comparative studies have identified a greater frequency of symptomatic lesions in patients with paraneoplastic GA compared to classic GA.7
References:
- Osto M, Smidi SA, Alnabolsi A, Rehman R, Potts G. An evidence-based approach for malignancy-associated and paraneoplastic generalized granuloma annulare. J Am Acad Dermatol. 2022;87(4):876-878. doi:10.1016/j.jaad.2021.11.051
- Müller CSL, Vogt T. Granuloma annulare – is it a paraneoplastic condition for malignant lymphoma?. J Dtsch Dermatol Ges. 2021;19(6):803-812. doi:10.1111/ddg.14401
- Joshi TP, Duvic M. Granuloma Annulare: An Updated Review of Epidemiology, Pathogenesis, and Treatment Options. Am J Clin Dermatol. 2022;23(1):37-50. doi:10.1007/s40257-021-00636-1
- Saber M, Khalili Tembi RS, Asilian A. Generalized granuloma annulare in a case of breast cancer: A case report and review of the literature. Clin Case Rep. 2021;9(10):e04980. Published 2021 Oct 18. doi:10.1002/ccr3.4980
- Garate D, Thang CJ, Damsky W, et al. Granuloma annulare is associated with an increased risk of hematologic malignancies: A multicenter cohort study using TriNetX. J Am Acad Dermatol. 2024;90(4):862-864. doi:10.1016/j.jaad.2023.12.028
- Bagci B, Karakas C, Kaur H, Smoller BR. Histopathologic Aspects of Malignancy-Associated Granuloma Annulare: A Single Institution Experience. Dermatopathology (Basel). 2023;10(1):95-103. Published 2023 Mar 4. doi:10.3390/dermatopathology10010015
- Mangold AR, Cumsky HJL, Costello CM, et al. Clinical and histopathologic features of paraneoplastic granuloma annulare in association with solid organ malignancies: A case-control study. J Am Acad Dermatol. 2018;79(5):913-920.e1. doi:10.1016/j.jaad.2018.06.022